Surgical Management of Charcot Spinal Arthropathy in the Face of Possible Infection
Int J Spine Surg. 2021 Aug;15(4):752-762. doi: 10.14444/8097.Epub 2021 Jul 27.
Alexander Von Glinski, Sven Frieler, Christopher J Elia, Darius Ansari, Clifford Pierre, Basem Ishak, Ronen Blecher, Bilal Qutteineh, Sarah Strot, Rod J Oskouian, Jens R Chapman
Abstract
Background: The design is a retrospective cohort study. Charcot spinal arthropathy (CSA) is a rare and poorly understood progressive destructive spine condition that usually affects patients with preexisting spinal cord injury. The complexity of this condition, especially when additionally burdened by superimposed infection in the CSA zone, can potentially lead to suboptimal management such as protracted antibiotic therapy, predisposition to hardware failure, and pseudarthrosis. While in noninfected CSA primary stabilization is the major goal, staged surgical management has not been stratified based upon presence of a superinfected CSA. We compare clinical and radiological outcomes of surgical treatment in CSA patients with and without concurrent spinal infections.
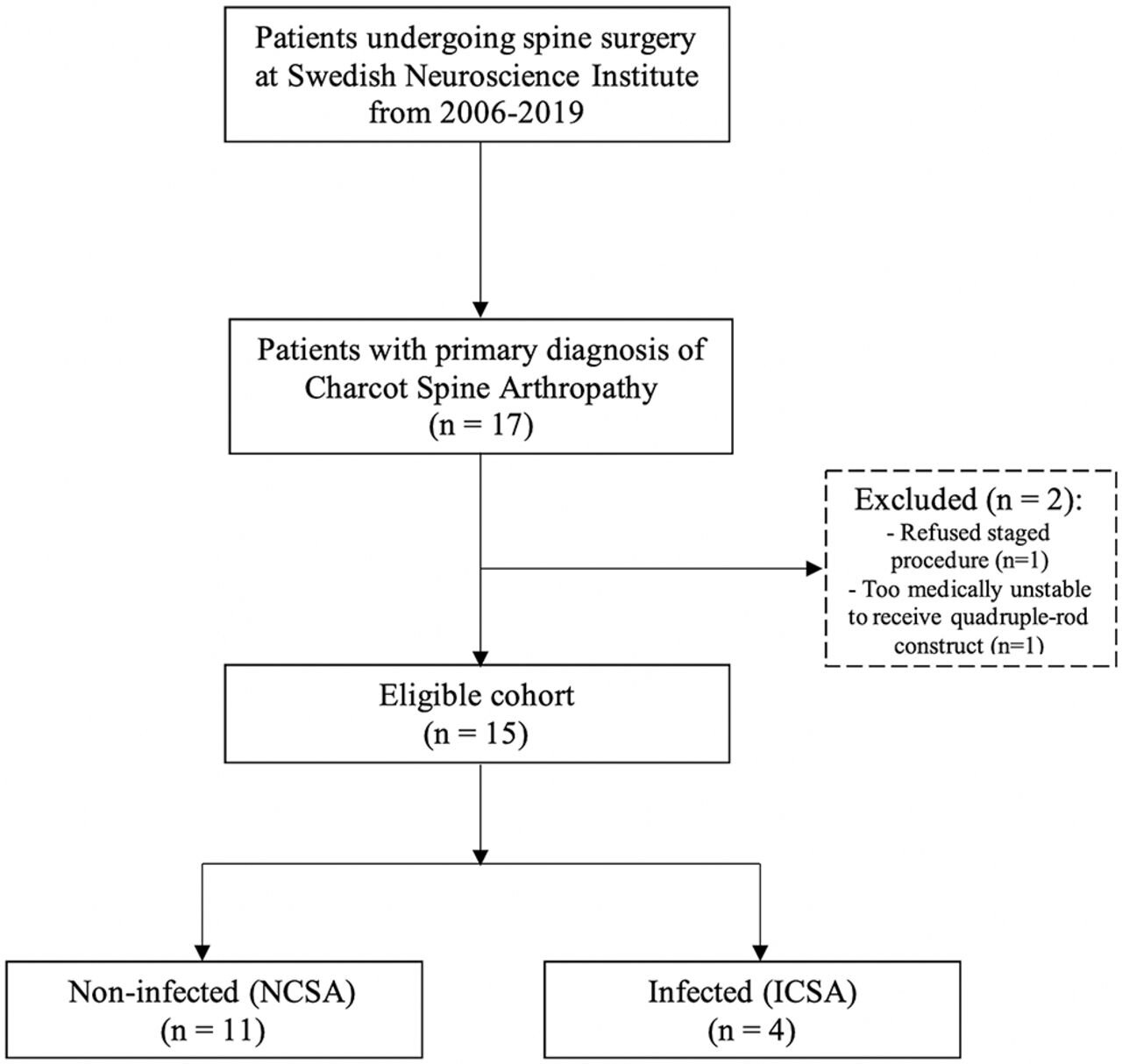
Methods: Our single-institution database was reviewed for all patients diagnosed with CSA and surgically treated, who were subsequently divided into 2 cohorts: spinal arthropathy with superimposed infection and those without. Those were comparatively studied for complications and reoperation rate.
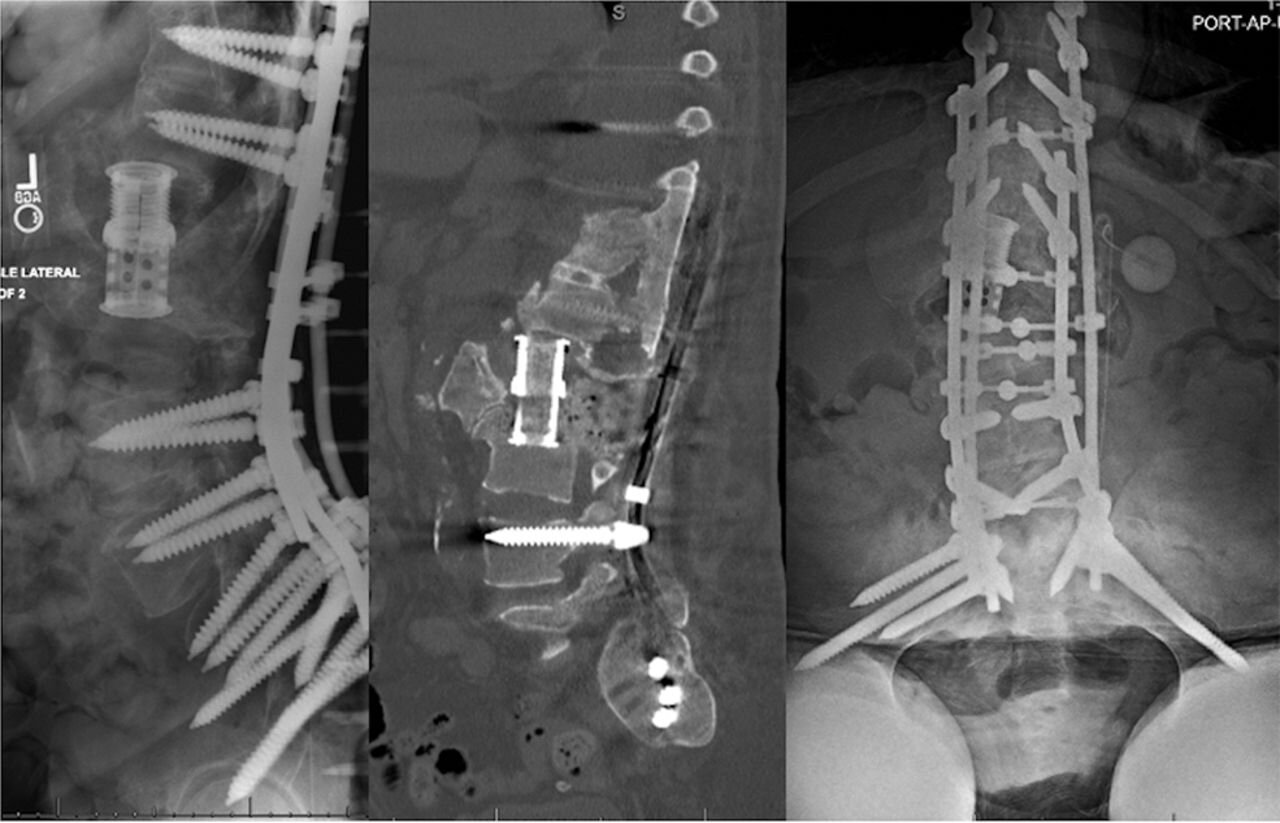
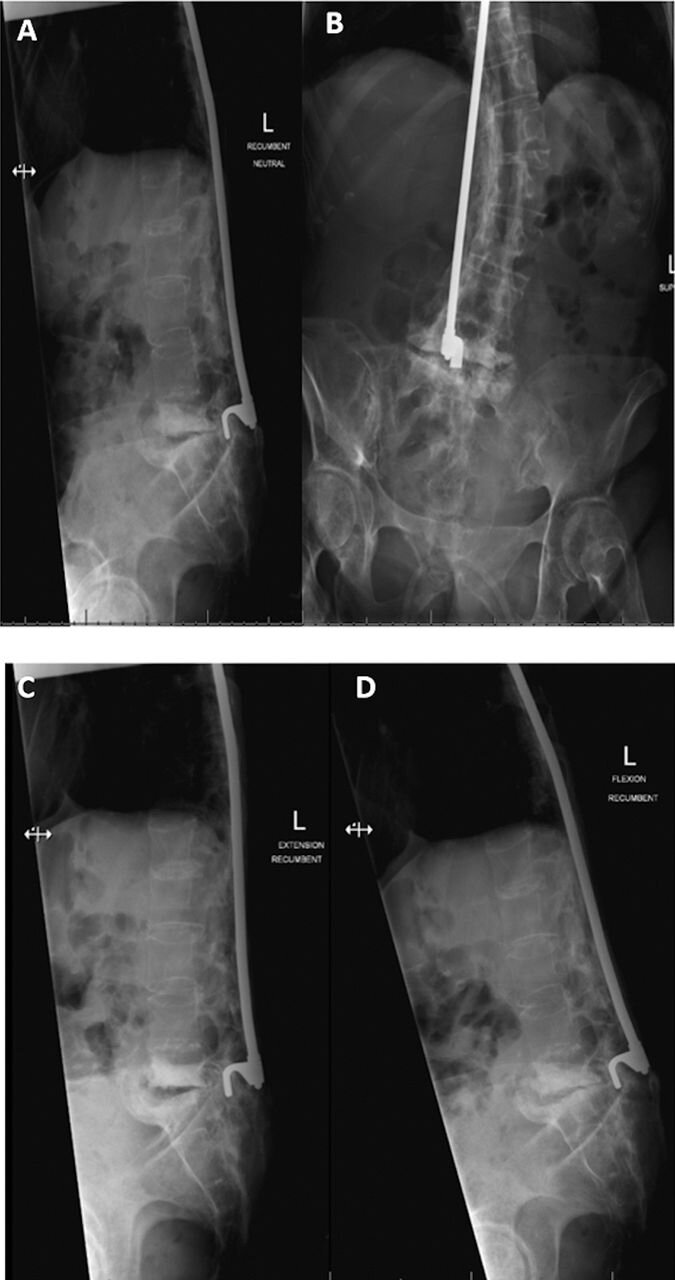
Results: Fifteen patients with CSA underwent surgical intervention; mean follow up of 15.3 months (range, 0-43). Eleven patients received stabilization with a quadruple-rod thoracolumbopelvic construct, while 4 patients with superinfected CSA underwent a staged procedure. Patients treated with a staged approach experienced fewer intraoperative complications (0% versus 18%) and fewer revision surgeries (25% versus 36%). Both cohorts had the same eventual healing.
Conclusions: Surgical management in CSA patients with primary emphasis on stability and modified surgical treatment based on presence of an active infection in the zone of neuropathic destruction will lead to similar eventual successful results with relatively few and manageable complications in this challenging patient population.
Level of evidence: 4.
Clinical relevance: The proposed treatment algorithm including the use of a quadruple-rod construct with lumbopelivic fixation and a staged approach in patients with superinfected CSA represents a reasonable option in the surgical treatment of CSA.
Keywords: Hounsfield unit (HU); bone morphogenic protein (BMP); polymethylmethacrylate (PMMA); quadruple-rod construct.