Abstract
INTRODUCTION:
Debilitating facial pain can seriously affect an individual's daily living. Given that the pathophysiology behind neuropathic and myofascial pain is not fully understood, when chronic facial pain goes undiagnosed, it has been proposed that one of the two is the likely cause. Since their discovery, glossopharyngeal neuralgia (GN) and Eagle's syndrome have been considered mostly conditions afflicting the adult population. However, when pediatric patients present with symptoms resembling GN or Eagle's syndrome, physicians are less apt to include these as a differential diagnosis simply due to the low prevalence and incidence in the pediatric population.
MATERIALS AND METHODS:
A literature review was performed with the aim to better understand the history of reported cases and to provide a comprehensive report of the anatomical variations that lead to these two conditions as well as the way these variations dictated medical and surgical management. Articles were obtained through Google Scholar and PubMed. Search criteria included key phrases such as pediatric glossopharyngeal neuralgia and pediatric Eagle syndrome. These key phrases were searched independently. PubMed was searched primarily then cross-referenced articles were found via Google Scholar. Results from non-English articles were excluded.
RESULTS:
A total of 58 articles were reviewed. Most of the articles focused on adult glossopharyngeal neuralgia, and the majority was comprised of case reports. When searched via PubMed, a total of 16 articles and 2 articles returned for glossopharyngeal neuralgia and Eagle's syndrome, respectively. After criteria selection and cross-referencing, a total of seven articles were found with respect to pediatric glossopharyngeal neuralgia.
CONCLUSIONS:
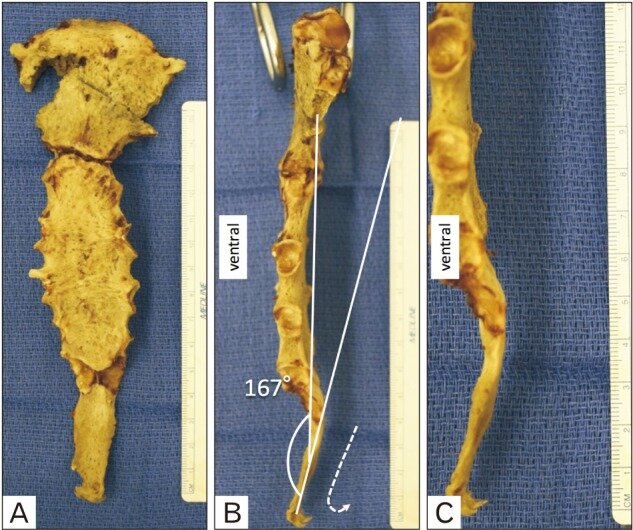
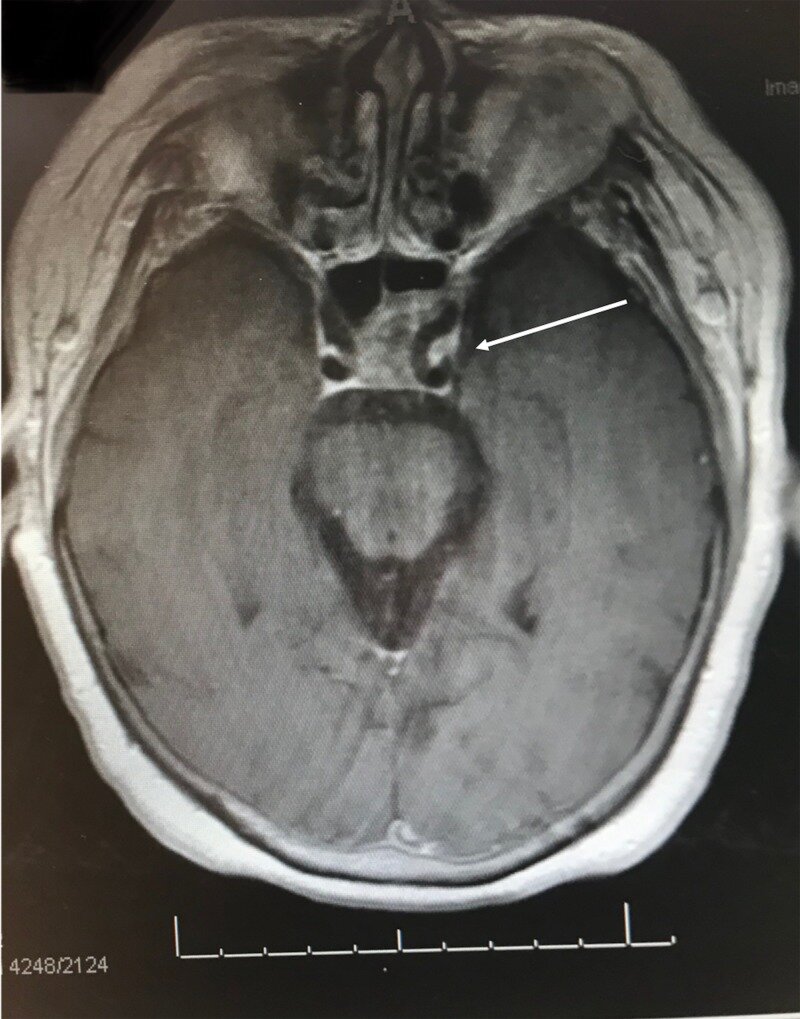
While they are rare conditions, there are multiple etiologies that lead to the debilitating symptoms of GN and Eagle's syndrome. The clinical anatomy proved notable as multiple causes of GN and Eagle's syndrome are due to variation in the anatomy of the neurovascular structures surrounding the glossopharyngeal nerve, an elongated styloid process, a calcified stylohyoid ligament as well as a calcified stylomandibular ligament. Due to the success of different treatment modalities, the treatment of choice is dependent on clinical judgment.
KEYWORDS:
Eagle’s syndrome; Gamma knife radiosurgery (GKRS); Glossopharyngeal neuralgia; Myofascial pain; Neuropathic; Trigeminal neuralgia